The Effect of Different Intensities of Static Stretching, as Measured by Hand-held Dynamometer, and the Relationship with Perceived Amount of Pain
정적스트레칭의 강도에 따른 효과 차이 및 통증 자각 정도와의 비교
Article information
Abstract
The purpose of this study was to examine the effect of different intensities of static stretching, as quantitatively measured with a hand-held dynamometer, on hamstring flexibility. The relationship between the intensity of static stretching and the amount of perceived pain was also investigated. Thirty-seven subjects participated and were randomly assigned into 3 groups. Stretch was performed with 3 different hand strength intensities as measured with a hand-held dynamometer for each group: 50 N in group 1, 70 N in group 2, and 90 N in group 3. Static stretching was performed once for 30 s. Active knee extension (AKE) was immediately measured and recorded as a post stretch value. Visual analogue scale (VAS) was also assessed at this time. After post-stretch measurement, additional AKE were collected at 2, 4, 6, 8, 10, 15, 20, 25, and 30 min. There were no significant differences in hamstring flexibility between groups with the intensity levels. The post-stretch values increased significantly after 2 min in group 1 (p=0.008) and after 6 min in group 2 (p=0.007) and group 3 (p=0.015). The mean VAS score was 5.2 in groups 1, 6.3 in group 2, and 6.3 in group 3. There was no correlation between VAS score and the effect of stretching (p=0.126). Our findings suggest that pain ratings might not be appropriate to determine the intensity of stretching and the use of hand-held dynamometer is highly recommended by the clinician or athletic trainer in the field because it can provide constant intensity of stretching.
Trans Abstract
이 연구는 정적 스트레칭의 강도 차이가 뒤넙다리근 유연성에 미치는 효과 및 강도에 따른 통증 자각정도 차이를 보고자 하였다. 피험자는 스트레칭 강도에 따라 무작위로 3가지 집단(50 N, 70 N, 90 N)으로 나뉘었다. 스트레칭 이후 피험자의 통증 자각 정도를 기록하였으며, 뒤넙다리근 유연성은 능동 무릎 폄 검사를 통해 측정하였다. 이때, 스트레칭 강도는 휴대용 근력계를 이용하여 측정하였다. 강도에 따른 유연성은 그룹간 유의미한 차이를 보이지 않았으나, 증가된 유연성의 감소는 50 N 그룹에서 가장 빠르게 관찰되었다. 또한, 스트레칭 강도는 통증 자각정도에 유의한 차이를 보이지 않았다. 주관적인 통증 자각 정도에 의존하기 보다는 휴대용 근력계를 이용한 정량적 스트레칭의 수행이 임상에서 추천될 수 있다.
Introduction
Hamstring flexibility plays an important role in maintaining postural balance and musculoskeletal function (Worrell et al., 1992), and is a key factor in increasing performance and preventing injury in sports (Rahnama et al., 2002; Gabbett 2004; Orchard et al., 2005). Most athletes who use the lower extremities are at high risk of a hamstring injury (Safran et al., 1989; Hartig et al., 1999). The hamstring muscle group consists of the biceps femoris, semitendinosus, and semimembranosus (Agre 1985). The hamstring muscle group acts at two joints, and plays a significant role in both knee flexion and hip extension (Kim MH, 2008). To prevent muscular injury, both warm-up and stretching exercises are used individually or together (Safran et al., 1989; Woods et al., 2007). Static, dynamic, ballistic, and proprioceptive neuromuscular facilitation (PNF) stretching have been widely used to increase hamstring flexibility (Halbertsma et al., 1999; Thacker et al., 2004; Ford et al., 2007). For PNF stretching, a combination of passive stretching, isometric contraction, relaxation, and passive stretching is generally used, and takes advantage of the neural properties of tissues (Spernoga et al., 2001; Amako et al., 2003). Dynamic stretching is a technique involving bouncing or jerking. Static stretching is a slow stretch technique that holds muscles in position for 6 to 60 seconds, to the point of discomfort (Bandy et al., 1994; Bandy et al., 1997; Roberts et al., 1999; Amako et al., 2003; Cipriani et al., 2003). As a result of extensive research, static stretching is most commonly used and is clinically proven. However, it has disadvantages in that the practitioner’s hand strength is not applied consistently and quantitative assessment is difficult (Woods et al., 2007). Since force in static stretching is simply estimated, each practitioner applies hand strength differently, which can diminish the effect of static stretching (Shrier 1999; Herbert et al., 2002; Weldon et al., 2003; Young et al., 2006). Practitioners usually adjust their hand strength by feel at the end range of motion and observe the patient’s pain response to stretching. As a result, flexibility may not be improved after application of static stretching if it is not enough to induce tissue deformity. On the contrary, muscles can be injured when overstressed. Therefore, hand strength is a key factor in determining the intensity of stretching and influencing its effectiveness.
In this study, hand strength while performing static stretching was measured with a hand-held dynamometer. A hand-held dynamometer is easy to use, light and portable, and can provide valuable hand strength data while performing static stretching. The participant’s pain response while stretching was assessed with the Visual Analogue Scale (VAS). The purpose of this study was to examine the effect of different intensities of static stretching, as quantitatively measured with a hand- held dynamometer, and their effect on sustained duration of hamstring flexibility. The relationship between the intensity of static stretching and the amount of perceived pain was also investigated.
Materials and Methods
1. Subjects
A convenience sample of university students was recruited and thirty-seven students participated in this experiment. Subjects with a previous history of trunk or lower extremity injury or any other significant disorder were excluded. Informed consent was obtained from all subjects prior to participating in the study.
2. Instrumentation
A standard goniometer was used to measure the range of knee extension. The hand-held dynamometer (MicroFET3, Hoggan Health Industries Co., UT, USA) measured strength intensities during stretching. The amount of pain perceived by the subject was measured using VAS (range 0∼10) after stretching.
3. Procedure
All experiments were performed with subjects in supine position. To measure knee extension angle with a goniometer, the lateral epicondyle of the femur, greater trochanter of the femur, and lateral malleolus of the fibula were marked before beginning the experiment. Each subject was positioned supine with the hip and knee 0° of flexion and then performed active knee extension (AKE) with 90° hip flexion. AKE measurement recorded was the angle between the full knee extension and leg position. Throughout the procedure, opposite lower extremity extended and maintained contact with an examination table and hip remained 0° of flexion. A metal frame was used to maintain 90° hip flexion (Fig. 1). All subjects performed 5 AKE warm-ups, and a 6th AKE was recorded for pre-stretch data. Subjects were randomly divided into group 1 (n=12), group 2 (n=13), and group 3 (n=12). Stretch was performed with 3 different hand strength intensities as measured with a hand-held dynamometer for each group: 50 N in group 1, 70 N in group 2, and 90 N in group 3. The hand-held dynamometer was placed under the heel and the practitioner maintained the constant target values of 50, 70, or 90 N by monitoring the values displayed on the screen of the device during stretching. Static stretching was performed once for 30 s. AKE was immediately measured and recorded as a post-stretch value. VAS was also assessed at this time. After post-stretch measurement, the subject was given a rest break without movement, and additional AKE data were collected at 2, 4, 6, 8, 10, 15, 20, 25, and 30 min.
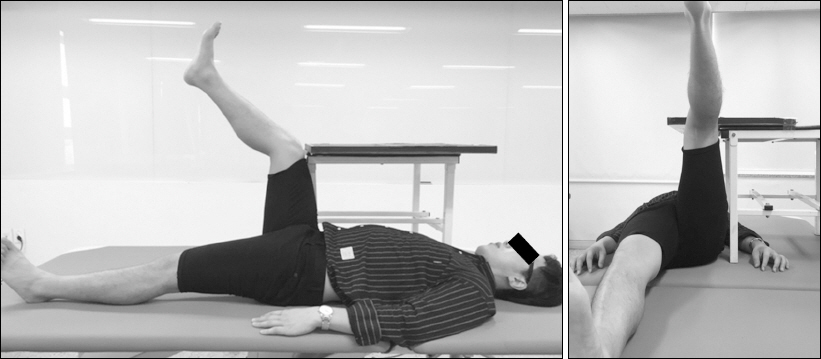
Subject performing active knee extension to measure hamstring flexibility.
4. Statistical analysis
Data analysis was performed using IBM SPSS version 23 for Windows. A repeated-measures analysis of variance was used to determine the differences for AKE across time. The Bonferroni test was used for pairwise differences. Spearman’s correlation coefficient was computed to quantify the relationship between VAS and post-stretch values. All values are presented as mean±standard deviation and statistical significance was set at p<0.05.
Results
Thirty-seven participants (18 men, 19 women, mean age 21.1±1.1 years, range=19.6∼24.3) were recruited for this experiment (Table 1) and there were no statistically significant differences in age, height, and body weight between groups. There were no significant differences in hamstring flexibility between group 1 and 2 (p=0.721), group1 and 3 (p=0.627), and group 2 and 3 (p=0.474) (Table 2). The post-stretch value showed the greatest decrease in group 3, but there was no significant difference in comparison with pre-stretch values (p=0.446) (Fig. 2). The post-stretch values increased significantly after 2 min in group 1 (p=0.008) and after 6 min in group 2 (p=0.007) and 3 (p=0.015). The pre-stretch values were significantly different only at 30 min (p=0.016) in group 1, 8 min (p=0.035) and 10 min (p=0.021) in group 2. AKE values in all groups showed rapid increase until 4 min after stretching. After 4 min, the values showed a gradual increase to an average 150.7% to 158.5% of pre-stretch values after 30 min. VAS score ranged from 5.2 to 6.3 and showed no significant difference between group 1 and 2 (p=0.186), group1 and 3 (p=0.109), and group 2 and 3 (p= 0.975) (Fig. 3). Although the intensity of stretching increased, VAS score did not increase further. The correlation between VAS score and the effect of stretching was not statistically significant (p=0.126).
Subjects characteristics
Mean values of active knee extension
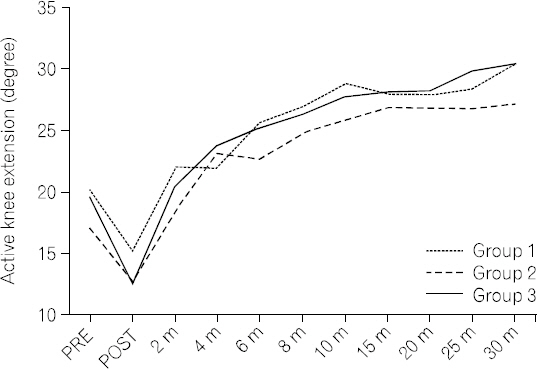
Longitudinal active knee extension measurements. PRE: Prestretch, POST: Post-stretch.

Changes in visual analogue scale depending on strength level measured by hand-held dynamometer.
Discussion
Hamstring stretch is widely used by both athletes and non-athletes. The intensity of hand strength while stretching is usually determined by the experience of the practitioner and the amount of pain perceived by the subject. However, stretching performed with high intensity using subjective criteria can easily cause unexpected injury. In this study, the intensity of stretching was quantitatively and precisely measured with a hand-held dynamometer based on an evaluation of the sustained effect of stretching according to intensity. The study showed that increased intensity of stretching did not result in a corresponding increase in hamstring flexibility, and the sustained effect was not statistically significant. Thus, hamstring flexibility was unaffected above a certain intensity. The intensity of 50 N and below might be sufficient to improve hamstring flexibility. Additionally, the amount of perceived pain during stretching and the intensity measured by the dynamometer were not statistically significant. This means that subjective pain ratings are not appropriate to determine the intensity of stretching.
In this study, the intensity of hand strength previously determined by subjective experience was successfully measured with a hand-held dynamometer, so that subjects performed stretching with constant intensity. Even though the intensity of stretching increased, the decrease in AKE values was limited, and there was no difference in the sustained effect between groups. This might be because the duration of stretching was insufficient to cause tissue deformation (Bandy et al., 1994; Webright et al., 1997; Bandy et al., 1998). Tissue with viscoelastic properties can undergo deformation when it moves through an elastic range to attain a plastic range according to stress-strain relationships (Stromberg et al., 1969; Taylor et al., 1990). Therefore, stimulation should be maintained for a certain period of time to achieve tissue deformation; however, short-duration stretch did not induce this change, and the results showed that sustained effect did not appear to make a significant difference. Additionally, the reduction of hamstring flexibility over time was compounded by the immediate effect of AKE warm-up and an increase in muscle stiffness due to inactivity after stretching, thus demonstrating thixotropic properties (Lakie et al., 1984; Hagbarth et al., 1985; Lakie et al., 1988; Walsh 1992). The AKE value at pre- stretch was higher than the value at 30 min because the AKEs performed before stretching temporarily enhanced hamstring flexibility and then gradually decreased over time.
In addition to the resistance at the end range of motion while stretching, the practitioner determines the intensity of stretching according to the subject’s response (Sullivan et al., 1992; Hartig et al., 1999; de Weijer et al., 2003). A subject’s feedback is a major factor in determining the intensity of stretching, but has not been fully studied. In this study, individual pain level corresponding to increasing intensity of stretching was assessed with the VAS. The average VAS score was 5.9±2.0 with average intensity of stretching, and increased intensity of stretching was not associated with an increase in VAS score. The VAS score with lower intensity stretching was not statistically different from the VAS score with higher intensity stretching. Therefore, a subject’s feedback is insufficient as an objective reference to determine the intensity of stretching, because it is strongly influenced by individual subjectivity (Dixon et al., 1981; Carlsson 1983; Miller et al., 1993).
Future study is needed to clarify the differences between groups with routine use of prolonged stimulation with variable intensity (Kim OH, 2009). In static stretching, it is generally known that using stretch for 30 s is beneficial, but is insufficient to induce tissue deformation and produce a sustained effect if a regular routine stretching program is not provided (Bandy et al., 1994; Bandy et al., 1997). Thus, the findings are limited by the short time and total duration of stretching in this study. Additionally, it is necessary to study tissue plasticity and characteristic changes with age through additional experiments in athletes and specific age groups, rather than in healthy adult men and women alone.
There was no significant difference in the effect of stretching with an increase in intensity for 30 s. There was also no statistically significant difference in sustained effect time between groups. In addition, increasing intensity of stretching did not raise individual pain levels. The findings in the present study suggest that mild to moderate stretching is highly recommended in preference to excessive stretching by the clinician or athletic trainer in the field, because there was no significant difference in the short-term effect with higher-intensity one-time stretching. The determination of the level of intensity of stretching also requires an objective measurement tool to quantify applied hand strength, rather than simply relying on a subject’s subjective pain level. The use of a hand-held dynamometer might prevent tissue damage caused by excessive stress by applying a consistent range of intensity, and thus ensures safety.